Signs and Symptoms: few. After exposure to high Ct, seizures, respiratory and cardiac arrest.
Detection: The M256A1 detector ticket detects hydrogen cyanide (AC) as vapor or gas in the air, and the M272 kit detects cyanide in water. The ICAD, M18A2, and M90 detectors also detect AC. The CAM, M8A1 automatic chemical agent alarm (ACAA), and M8 and M9 paper do not detect cyanide.
Decontamination: Skin decontamination is usually not necessary because the agents are highly volatile. Wet, contaminated clothing should be removed and the underlying skin decontaminated with water or other standard decontaminates.
Management: Antidote: intravenous (IV) sodium nitrite and sodium thiosulfate. Supportive: oxygen, correct acidosis.
Cyanide is a rapidly acting lethal agent that is limited in its military usefulness by its high LCt50 and high volatility. Death occurs within six to eight minutes after inhalation of a high Ct. Sodium nitrite and sodium thiosulfate are effective antidotes.
HISTORY/MILITARY RELEVANCE
The French used about 4000 tons of cyanide in World War I without notable military success, possibly because the small one- to two-pound munitions used could not deliver the large amounts needed to cause biological effects. Other factors included the high volatility of cyanide (which quickly evaporated and dispersed) and its "all or nothing" biological activity, i.e., it caused few effects below the lethal Ct (in contrast to mustard, which causes eye damage at 1% of the lethal amount).
The U.S. maintained a small number of cyanide munitions during World War II. Japan allegedly used cyanide against China before and during World War II, and Iraq may have used cyanide against the Kurds in the 1980s.
Terms. The term cyanide refers to the anion CN-, or to its acidic form, hydrocyanic acid (HCN). Cyanogen (C2N2) is formed by the oxidation of cyanide ions; however, the term cyanogen has also come to refer to a substance that forms cyanide upon metabolism and produces the biological effects of free cyanide (the term cyanogen is from "cyano" and "gennan," Greek meaning "to produce"). A simple cyanide (HCN, NaCN) is a compound that dissociates to the cyanide anion (CN-) and a cation (H+, Na+). A nitrile is an organic compound that contains cyanide. A cyanogen usually refers to a nitrile that liberates the cyanide anion during metabolism and produces the biological effects of the cyanide anion. Cyanogens may be simple (cyanogen chloride) or complex (sodium nitroprusside).
Cyanides are also called "blood agents," an antiquated term still used by many in the military. At the time of the introduction of cyanide in World War I, the other chemical agents in use caused mainly local effects. Riot-control agents injured the skin and mucous membranes from direct contact, and phosgene damaged the lungs after inhalation. In contrast, inhaled cyanide produces systemic effects and was thought to be carried in the blood; hence the term "blood agent." The widespread distribution of absorbed nerve agents and vesicants via the blood invalidates this term as a specific designator for cyanide. Also, the use of "blood agent" also carries the connotation that the main site of action of cyanide is in the blood, whereas cyanide acts primarily outside the bloodstream.
Materials of interest as chemical agents are the cyanide hydrogen cyanide (hydrocyanic acid, AC) and the simple cyanogen, cyanogen chloride (CK). Cyanogen bromide was used briefly in World War I, but is of no present interest.
Sources other than military. The cyanide ion is ubiquitous in nearly all living organisms that tolerate and even require the ion in low concentrations. The fruits and seeds (especially pits) of many plants, such as cherries, peaches, almonds, and lima beans contain cyanogens capable of releasing free cyanide following enzymatic degradation. The edible portion (the roots) of the cassava plant (widely used as a food staple in many parts of the world) is also cyanogenic. The combustion of any material containing carbon and nitrogen has the potential to form cyanide; some plastics (particularly acrylonitriles) predictably release clinically significant amounts when burned. Industrial concerns in the U.S. manufacture over 300,000 tons of hydrogen cyanide annually. Cyanides find widespread use in chemical syntheses, electroplating, mineral extraction, dyeing, printing, photography, and agriculture, and in the manufacture of paper, textiles, and plastics.
PHYSICOCHEMICAL CHARACTERISTICS
The cyanides exist as liquids in munitions but rapidly vaporize upon detonation of the munitions. The major threat is from the vapor. The liquid toxicity is approximately that of mustard (see toxicity, below).
The preferred way to deliver cyanide is by large munitions (bombs, large shells), because smaller weapons will not provide the concentrations needed for effects.
The immediately-dangerous-to-life-and-health (IDLH) concentration of hydrogen cyanide (AC) is 50.0 parts per million (ppm); that for cyanogen chloride (CK) is 0.6 mg/m3. M8 paper, M9 paper, the CAM, ACAMS, M8A1 automatic chemical-agent detector alarm, and DAAMS are incapable of detecting cyanide either as AC or CK. However, the following detectors have the capacity to detect AC and CK at the threshold limits given:
DETECTOR |
AC |
CK |
M256A1 |
7.0 mg/m3 |
|
M272 (in water) |
20.0 mg/m3 |
|
MINICAMS |
|
130 ppbv |
Draeger |
|
0.25 - 5 ppm |
ICAD |
250 mg/m3 |
|
M18A2 |
8.0 mg/m3 |
|
M90 |
30 mg/m3 |
|
M93A1 Fox |
|
46 mg/m3 |
Because the odor of cyanide may be faint or lost after accommodation, olfactory detection of the odor of bitter almonds is not a reliable indicator of phosgene exposure, even for those who possess the gene required to smell cyanide. The activated charcoal in the canister of the chemical protective mask adsorbs cyanide, and the mask affords full protection from this gas.
Cyanide salts in solid form or in solution are readily absorbed from the gastrointestinal tract when ingested. Moreover, the lower the pH in the stomach, the more hydrogen cyanide is released as gas from ingested salts. Liquid cyanide and cyanide in solution can be absorbed even through intact skin, but this route of entry is usually not clinically significant. Parenteral absorption of liquid cyanide can also occur from wounds. Cyanide is readily absorbed through the eyes, but the most important route of entry in a battlefield or terrorist scenario would likely be by inhalation. Following absorption, cyanide is quickly and widely distributed to all organs and tissues of the body. Ingestion leads to particularly high levels in the liver when compared with inhalation exposure, but both routes lead to high concentrations in plasma and erythrocytes and in the heart, lungs, and brain.
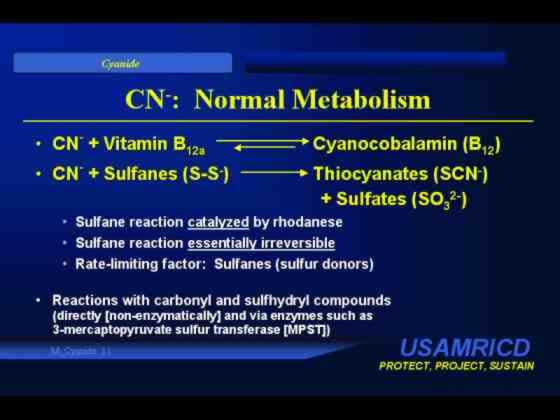
An example of the ability of cyanide to react with metals in the body is its reaction with the cobalt in hydroxycobalamin (vitamin B12a) to form cyanocobalamin (vitamin B12). The reactions of cyanide with metals are reversible and exhibit concentration-dependent equilibria, but he reactions of cyanide with sulfur-containing compounds are catalyzed by the enzyme rhodanese (EC 2.8.I.1) and are essentially one-way and irreversible. The rate-limiting factor in the rhodanese-mediated reactions is usually the availability of sulfur donors in the body. These reactions can be accelerated therapeutically by providing a sulfane such as sodium thiosulfate. The reaction products, thiocyanates and sulfites, are significantly less toxic than cyanide itself and are eliminated in the urine. Cyanide also reacts with carbonyl and sulfhydryl groups (directly or via 3-MPST and other enzymes). However, the two most important kinds of reactions from the perspective of understanding the classical mechanism of action of cyanide and its response to specific antidotal therapy are the reactions with metals and the enzyme-catalyzed reactions with sulfur-containing compounds.
Cyanide is eliminated unchanged from the body in breath, sweat, and urine - as sodium thiocyanate in the urine and as iminothiocarboxyllic acid (ITCA) from reaction with sulfhydryl groups. High concentrations of cyanide in the body will also lead to measurable increases in urinary elimination of cyanocobalamin (vitamin B12).
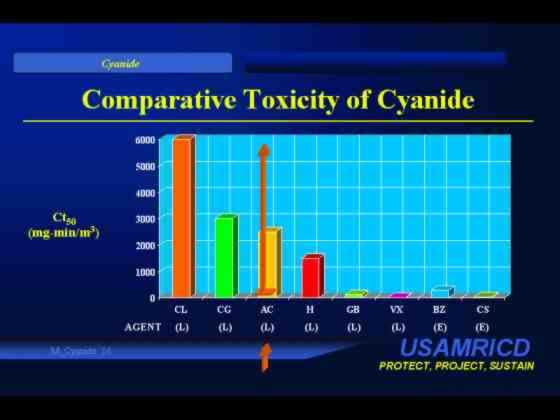
Cyanide is the least toxic of the "lethal" chemical agents. The LCt50s of AC and CK by inhalation have been estimated to be 2500-5000 mg·min/m3 for AC and about 11,000 mg·min/m3 for CK. LD50s for hydrogen cyanide have been estimated to be 1.1 mg/kg for IV administration and 100 mg/kg after skin exposure. The oral LD50s for sodium and potassium cyanide are about 100 and 200 mg/kg, respectively.
Cyanide is unique among military chemical agents because it is detoxified at a rate that is of practical importance, about 17 mcg/kg·min. As a result the LCt50 is greater for a long exposure (e.g., 60 minutes) than for a short exposure (e.g., 2 minutes).
TOXICODYNAMICS (MECHANISM OF ACTION)
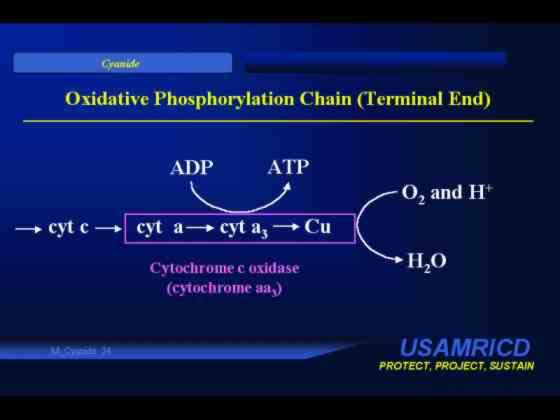
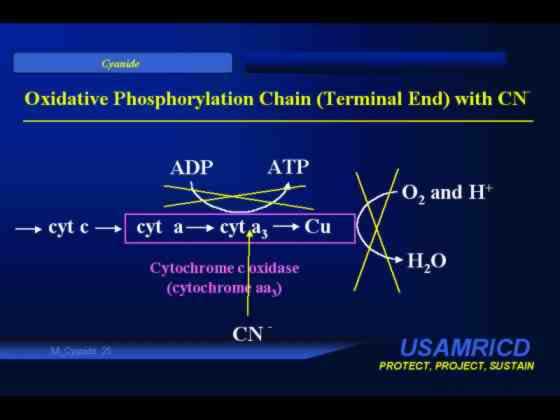
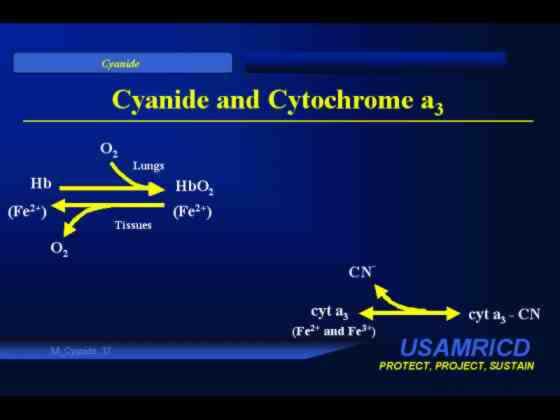
Cyanide has a high affinity for certain sulfur compounds (sulfanes, which contain two covalently bonded but unequally charged sulfur atoms) and for certain metallic complexes, particularly those containing cobalt and the trivalent form of iron (Fe3+). The cyanide ion can rapidly combine with iron in cytochrome a3 (a component of the cytochrome aa3 or cytochrome oxidase complex in mitochondria) to inhibit this enzyme, thus preventing intracellular oxygen utilization. The cell then utilizes anaerobic metabolism, creating excess lactic acid and a metabolic acidosis. Cyanide also has a high affinity for the ferric iron of methemoglobin, and one therapeutic stratagem induces the formation of methemoglobin to which cyanide preferentially binds.
The small quantity of cyanide always present in human tissues is metabolized at the approximate rate of 17 mcg/kg·min, primarily by the hepatic enzyme rhodanese, which catalyzes the irreversible reaction of cyanide and a sulfane to produce thiocyanate, a relatively nontoxic compound excreted in the urine. (An elevated concentration of thiocyanate in either blood or urine is evidence of cyanide exposure.) The limiting factor under normal conditions is the availability of a sulfane as a substrate for rhodanese, and sulfur is administered therapeutically as sodium thiosulfate to accelerate this reaction. The lethal dose of cyanide is time dependent because of the ability of the body to detoxify small amounts of cyanide via the rhodanese-catalyzed reaction with sulfane. A given amount of cyanide absorbed slowly may cause no biological effects even though the same amount administered over a very short period of time may be lethal. In contrast, the LCt50 of each of the other chemical agents, which are not metabolized to the same extent as is cyanide, is relatively constant over time. A lethal amount causes death whether administered within minutes or over hours.
The organs most susceptible to cyanide are the central nervous system (CNS) and the heart. Most clinical effects are of CNS origin and are nonspecific.
Approximately 15 seconds after inhalation of a high concentration of cyanide, there is a transient hyperpnea, followed within in 15 to 30 seconds by the onset of convulsions. Respiratory activity stops two to three minutes later, and cardiac activity ceases several minutes later still, or approximately six to eight minutes after exposure.
The onset and progression of signs and symptoms after ingestion of cyanide or after inhalation of a lower concentration of vapor are slower. The first effects may not occur until several minutes after exposure, and the time course of these effects depends on the amount absorbed and the rate of absorption. The initial transient hyperpnea may be followed by feelings of anxiety or apprehension, agitation, vertigo, a feeling of weakness, nausea with or without vomiting, and muscular trembling. Later, consciousness is lost, respiration decreases in rate and depth, and convulsions, apnea, and cardiac dysrhythmias and standstill follow. Because this cascade of events is prolonged, diagnosis and successful treatment are possible.
The effects of cyanogen chloride include those described for hydrogen cyanide. Cyanogen chloride is also similar to the riot-control agents in causing irritation to the eyes, nose, and airways, as well as marked lacrimation, rhinorrhea, and bronchosecretions.
Physical Findings. Physical findings are few and nonspecific. The two that are said to be characteristic are in fact not always observed. The first is severe respiratory distress in an acyanotic individual. When seen, "cherry-red" skin suggests either circulating carboxyhemoglobin from carbon monoxide poisoning or high venous oxygen content from failure of extraction of oxygen by tissues poisoned by cyanide or hydrogen sulfide. However, cyanide victims may have normal appearing skin and may even be cyanotic, although cyanosis is not classically associated with cyanide poisoning.
Table: Cyanide (AC and CK) Effects from Vapor Exposure
|
Moderate, from low concentration |
Transient increase in rate and depth of breathing, dizziness, nausea, vomiting, headache. |
These may progress to severe effects if exposure continues. |
The time of onset of these effects depends on the concentration but is often within minutes after onset of exposure. |
|
Severe, from high concentration |
Transient increase in rate and depth of breathing -- 15 seconds. Convulsions -- 30 seconds. Cessation of respiration -- 2 to 4 minutes. Cessation of heartbeat -- 4 to 8 minutes. |
|
|
In addition to the preceding effects, CK causes intense irritation of the eyes, nose, and airways.
The second classic sign is the odor of bitter almonds; however, approximately 50% of the population are genetically unable to detect the odor of cyanide.
The casualty may be diaphoretic with normal sized or large pupils. A declining blood pressure and tachycardia follow an initial hypertension and compensatory bradycardia. Terminal hypotension is accompanied by bradyarrhythmias before asystole.
Effects begin 15 seconds following inhalation of a lethal Ct; death ensues in 6 to 8 minutes. The onset of effects following inhalation of lower Cts may be as early as minutes after the onset of exposure. After exposure is terminated by evacuation to fresh air or by masking, there is little danger of delayed onset of effects.
Battlefield inhalation exposure to either cyanide or a nerve agent may precipitate the sudden onset of loss of consciousness followed by convulsions and apnea. The nerve agent casualty has miosis (until shortly before death), copious oral and nasal secretions, and muscular fasciculations. The cyanide casualty has normal sized or dilated pupils, few secretions, and muscular twitching, but no fasciculations. In addition, the nerve agent casualty may be cyanotic, and the cyanide casualty usually is not.
1. An elevated blood cyanide concentration. Mild effects may be apparent at concentrations of 0.5-1.0 mcg/ml, and concentrations of 2.5 mcg/ml and higher are associated with coma, convulsions and death.
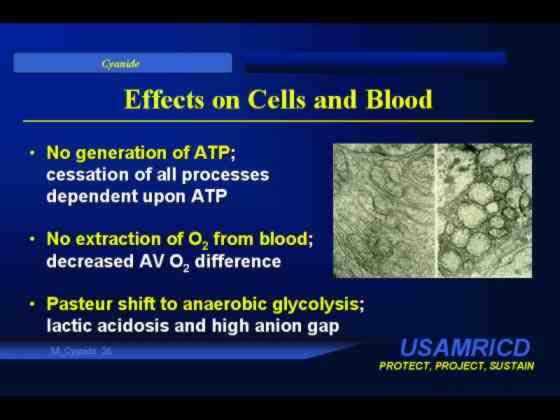
2. Acidosis. Metabolic acidosis with a high concentration of lactic acid (lactic acidosis) or a metabolic acidosis with an unexplained high anion gap (if the means to measure lactic acid are not available) may be present. Because oxygen cannot be utilized, anaerobic metabolism with the production of lactic acid replaces aerobic metabolism. Lactic acidosis, however, may reflect other disease states and is not specific for cyanide poisoning.
3. Oxygen content of venous blood greater than normal. This also is a result of poisoning of the intramitochondrial respiratory chain and the resulting failure of cells to extract oxygen from arterial blood. This finding is also not specific for cyanide poisoning.
Management of cyanide poisoning begins with removal to fresh air. Dermal decontamination is unnecessary if exposure has been only to vapor, but wet clothing should be removed and the underlying skin should be washed with soap and water or water alone if liquid on the skin is a possibility. Attention to the basics of intensive supportive care is critical and includes mechanical ventilation as needed, circulatory support with crystalloids and vasopressors, correction of metabolic acidosis with IV sodium bicarbonate, and seizure control with benzodiazepine administration. The fact that cyanide inhibits cellular utilization of oxygen would lead to the expectation that supplemental oxygen would not be of use in cyanide poisoning. However, in fact, administration of 100% oxygen has been found empirically to exert a beneficial effect and should be a part of general supportive care for every cyanide-poisoned patient.
Symptomatic patients, especially those with severe manifestations, may further benefit from specific antidotal therapy. This is provided in a two-step process. First, a methemoglobin-forming agent such as amyl nitrite (available in civilian antidote kits, but not in military kits, as crushable ampoules for inhalation) or sodium nitrite (for IV use) is administered, since the ferric ion (Fe3+) in methemoglobin has an even higher affinity for cyanide than does cytochrome a3. The equilibrium of this reaction causes dissociation of bound cyanide from cytochrome a3 and frees the enzyme to help produce ATP again. The orthostatic hypotension produced by nitrite administration is not usually a concern in a severely intoxicated and prostrate cyanide casualty, but overproduction of methemoglobin may compromise oxygen-carrying capacity. Thus, nitrite is relatively contraindicated in, for example, smoke-inhalation victims. The initial adult dose, equivalent to one of the two sodium nitrite vials in the standard Pasadena (formerly Lilly) Cyanide Antidote Kit, is 10 ml. Pediatric nitrite dosing (in the case of a military response to a civilian terrorist incident) is dependent on body weight and hemoglobin concentration. The recommended pediatric dose, assuming a methemoglobin concentration of 12 g/dl, is 0.33 ml/kg of the standard 3% solution given slowly, IV, over 5 to 10 minutes.
The second step is provision of a sulfur donor, typically sodium thiosulfate, which is utilized as a substrate by rhodanese for its conversion of cyanide to thiocyanate. Sodium thiosulfate itself is efficacious, relatively benign, and also synergistic with oxygen administration and thus may be used without nitrites empirically in situations such as smoke inhalation with high carboxyhemoglobin levels. The initial adult dose, equivalent to one of the two large bottles in the Pasadena Kit, is 50 ml. The initial thiosulfate dose for pediatric patients is 1.65 ml/kg of the standard 25% solution, IV. Second treatments with each of the two antidotes may be given at up to half the original dose if needed.
It is important to realize that, although the combination of sodium nitrite and sodium thiosulfate may save victims exposed to 10 to 20 lethal doses of cyanide and are effective even after breathing has stopped, many patients will recover even without specific antidotal treatment if vigorous general supportive care is emphasized. Lack of availability of antidotes is therefore not a reason to consider even apneic cyanide casualties expectant. It is also important to realize that administration of antidotes, especially if not given slowly enough or if given in extremely large doses, is also associated with morbidity and even mortality. Antidotes should not be withheld in a patient in whom cyanide poisoning is suspected, but infusion rates should be slow and the drugs should be titrated to effect. Overdosage should be avoided.
Several alternative therapies are experimental antidotes are used in other NATO countries. Germany uses dimethylaminophenol (DMAP), a rapid methemoglobin former developed for intramuscular (IM) use. However, muscle necrosis at the site of injection occurs, and only the IV route of administration is recommended.
Certain cobalt compounds directly chelate cyanide to reduce its toxicity. Because cobalt compounds do not depend upon the formation of methemoglobin, they may exert their antidotal activity more quickly than do methemoglobin formers. Great Britain and France use cobalt edetate (Kelocyanor), but clear superiority to the methemoglobin formers has not been demonstrated, and cobalt toxicity is occasionally seen, particularly if the patient has only a mild exposure. The other cobalt compound sometimes used in France is hydroxycobalamin (vitamin B12a), which complexes with cyanide on a molar basis. Clinical trials of this compound are underway in the U.S.
Ongoing research is examining whether slow methemoglobin formers can be used as pretreatment to induce clinically asymptomatic methemoglobinemia in troops at high risk for cyanide exposure.
An immediate casualty is one who presents within minutes of inhalation exposure with convulsions or the recent onset of apnea, but with circulation intact. Immediate antidote administration will be lifesaving.
A minimal casualty is one who has inhaled less than a lethal amount and has mild effects. The antidotes may reduce his symptoms, but are not lifesaving.
The delayed casualty is one recovering from mild effects or successful therapy. Generally, it will be hours before full recovery. Evacuation is not necessary but might be considered until full recovery takes place.
An expectant casualty is apneic with circulatory failure.
Generally, a casualty who has had inhalation exposure and survives long enough to reach medical care will need little treatment.
Full recovery is usually relatively fast after cyanide intoxication. Those with mild to moderate effects from the agent can usually return to duty within hours, and those successfully treated after severe effects can return within a day.
|
Introduction |
Cyanide |
||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}