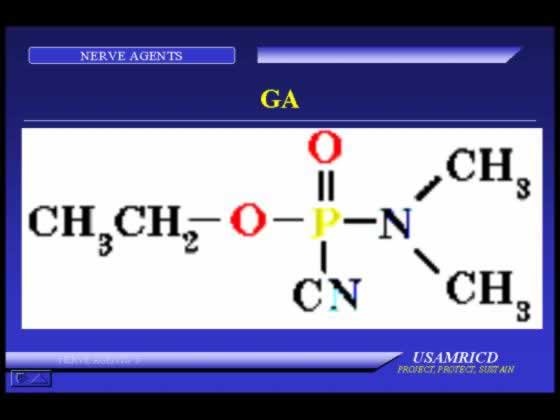
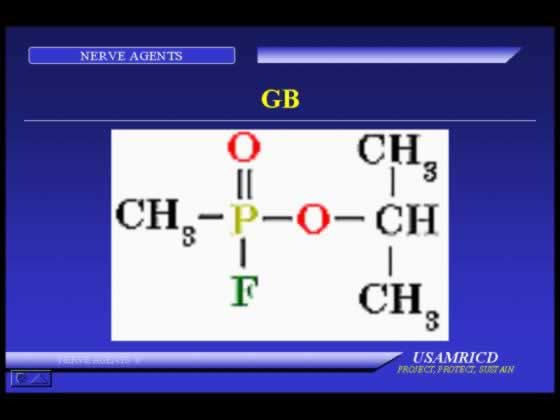
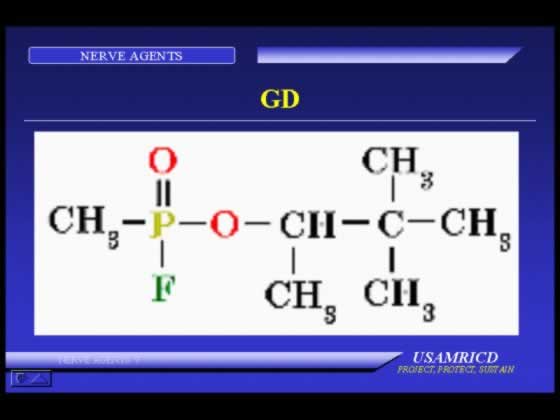
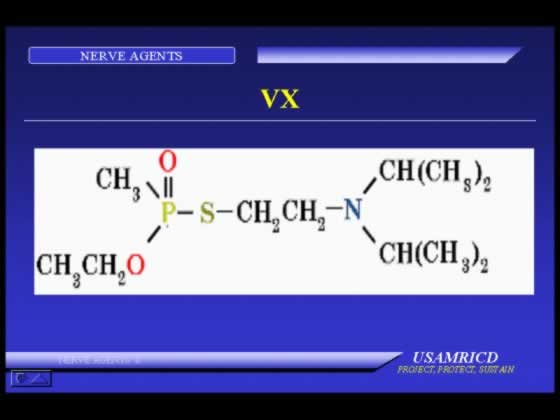
GA, GB, GD, GF, VX
Vapor:
Small exposure -- miosis, rhinorrhea, mild difficulty breathing. |
Large exposure -- sudden loss of consciousness, convulsions, apnea, flaccid paralysis, copious secretions, miosis. |
Liquid on skin:
Small to moderate exposure -- localized sweating, nausea, vomiting, feeling of weakness. |
Large exposure -- sudden loss of consciousness, convulsions, apnea, flaccid paralysis, copious secretions. |
Detection: M256A1, CAM, M8 paper, M9 paper, M8A1 and M8 alarm systems.
Decontamination: M291, M258A1, hypochlorite, large amounts of water.
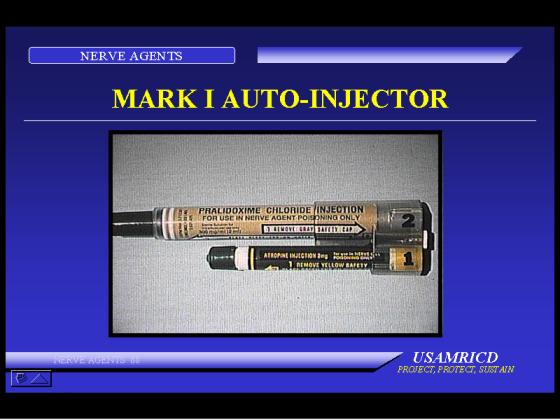
Immediate management: administration of MARK I Kits (atropine and pralidoxime chloride); diazepam in addition if casualty is severe; ventilation and suction of airways for respiratory distress.
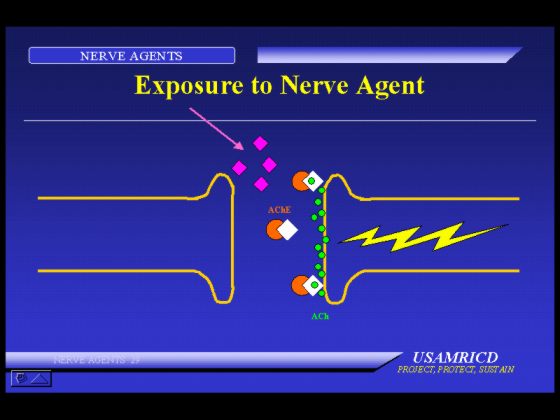
Nerve agents are the most toxic of the known chemical agents. They are hazards in their liquid and vapor states and can cause death within minutes after exposure. Nerve agents inhibit acetylcholinesterase in tissue, and their effects are caused by the resulting excess acetylcholine.
Nerve agents were developed in pre-World War II Germany. Germany had stockpiles of nerve agent munitions during World War II, but did not use them for reasons that are still unclear. In the closing days of the war, the United States and its allies discovered these stockpiles, developed the agents, and manufactured nerve agent munitions. The United States' chemical agent stockpile contains the nerve agents sarin (GB) and VX.
Nerve agents are considered major military threat agents. The only known battlefield use of nerve agents was in the Iraq-Iran conflict. Intelligence analysts indicate that many countries have the technology to manufacture nerve agent munitions.
Nerve agents are liquids under temperate conditions. When dispersed, the more volatile ones constitute both a vapor and a liquid hazard. Others are less volatile and represent primarily a liquid hazard. The "G-agents" are more volatile than VX. Sarin (GB) is the most volatile, but it evaporates less readily than water. GF is the least volatile of the G-agents. (GA, GB, GD, VX)
Nerve agents can be dispersed from missiles, rockets, bombs, howitzer shells, spray tanks, land mines, and other large munitions.
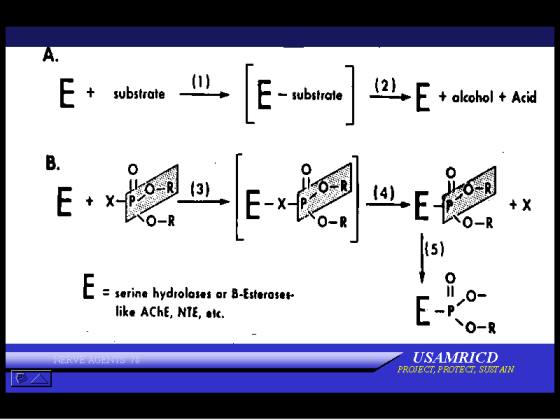
Nerve agents are organophosphorous cholinesterase inhibitors. They inhibit the butyrylcholinesterase in the plasma, acetylcholinesterase on the red cell, and acetylcholinesterase at cholinergic receptor sites in tissue. The three enzymes are not the same; even the two acetylcholinesterases have slightly different properties, although both have a high affinity for acetylcholine. The blood enzymes provide an estimate of the tissue enzyme activity. After acute exposure to a nerve agent, the erythrocyte enzyme activity most closely reflects the activity of the tissue enzyme, but during recovery the plasma enzyme activity more closely parallels tissue enzyme activity.
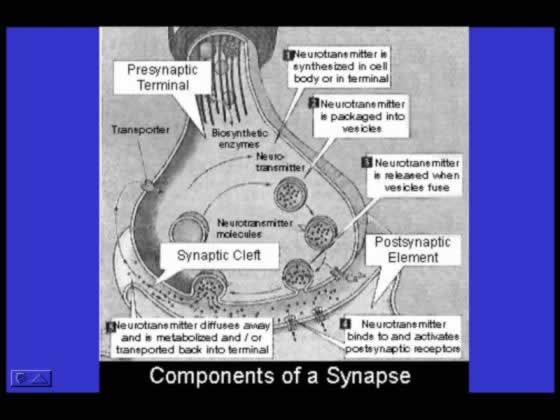
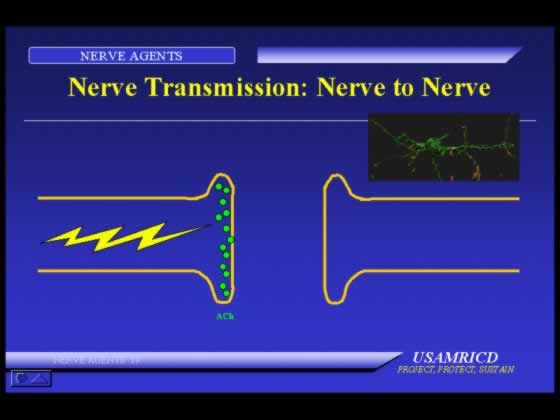
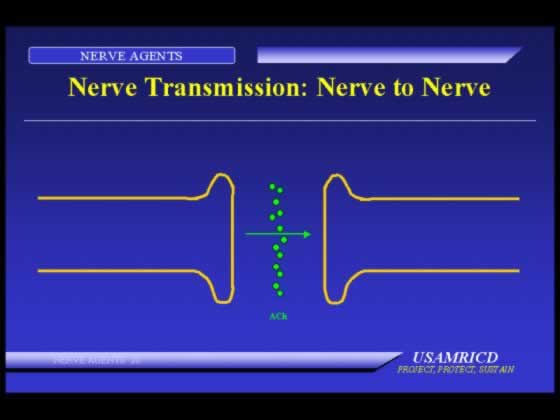
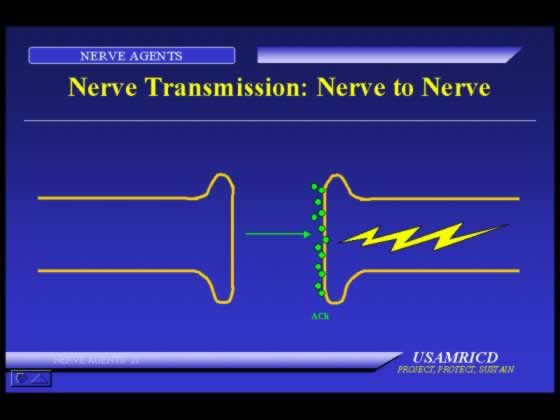
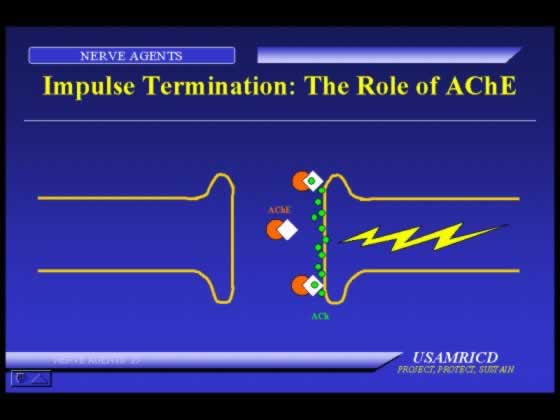
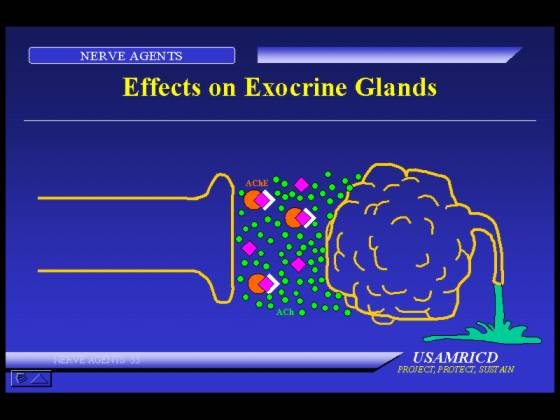
After a nerve agent inhibits the tissue enzyme, the enzyme cannot hydrolyze acetylcholine, the neurotransmitter, at cholinergic receptor sites. Acetylcholine accumulates and continues to stimulate the affected organ. The clinical effects from nerve agent exposure are caused by excess acetylcholine.
Neuromuscular Junction- The most common cholinergic synapse
Normal Cholinergic Signaling and the Role of Acetycholinesterase in Terminating the Action
Effects of Unopposed Excess Acetycholine
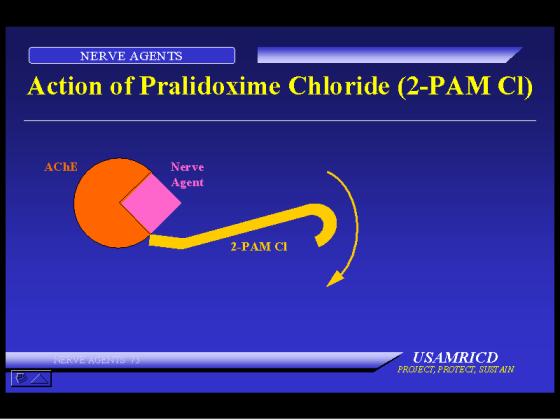
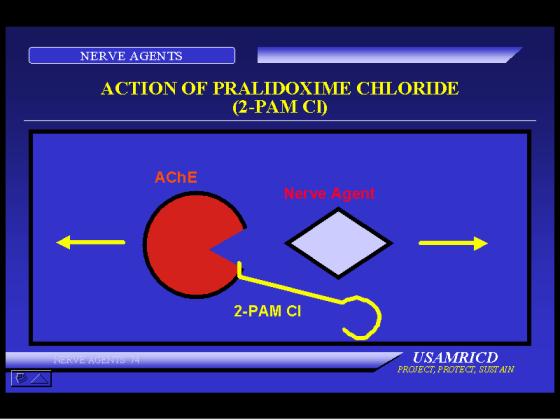
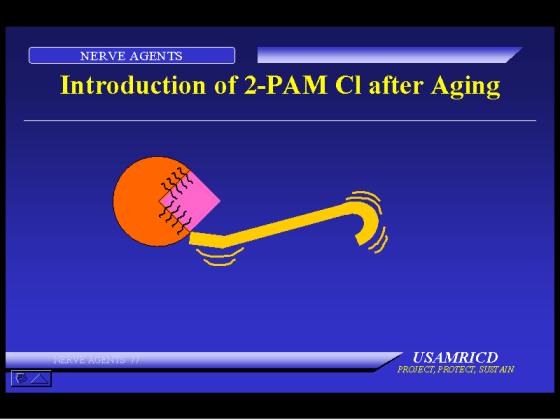
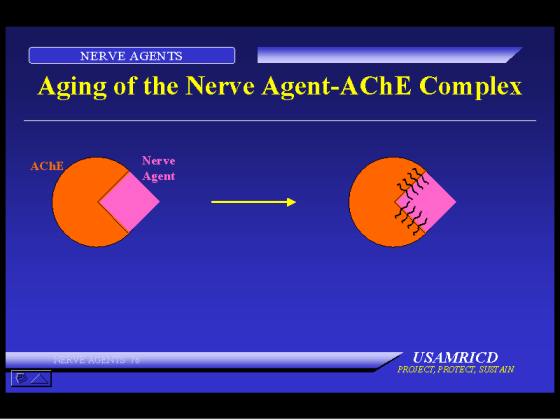
The attachment of the agent to the enzyme is permanent (unless removed by therapy). Erythrocyte enzyme activity returns at the rate of erythrocyte turnover, about 1% per day. Tissue and plasma enzyme activities return with synthesis of new enzymes. The rate of return of the tissue and plasma enzymes is not the same, nor is the rate the same for all tissue enzymes. However, the agent can be removed from the enzyme and the enzyme "reactivated" by several types of compounds, the most useful of which are the oximes. If the agent-enzyme complex has not "aged," oximes are useful therapeutically. Aging is a biochemical process by which the agent-enzyme complex becomes refractory to oxime reactivation of the enzyme. For most nerve agents, the aging time is longer than the time within which acute casualties will be seen. However, the aging time of the GD-enzyme complex is about two minutes, and the usefulness of oximes in GD poisoning is greatly decreased.
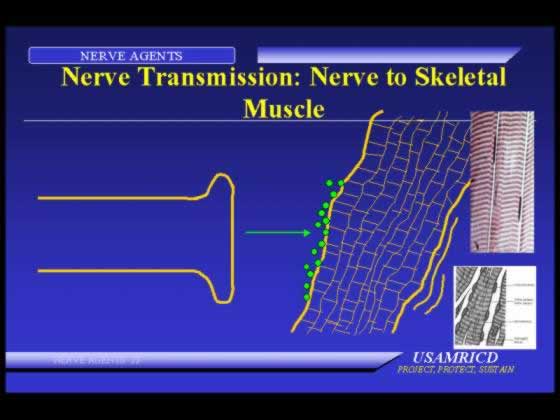
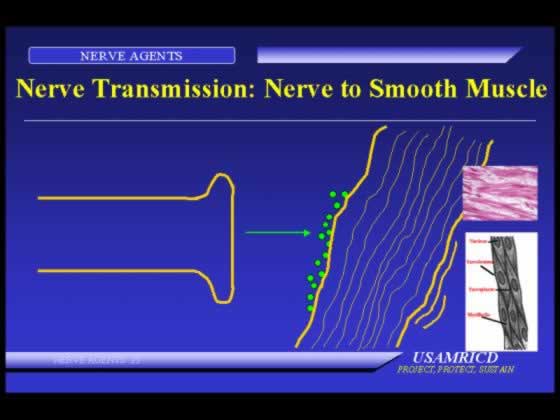
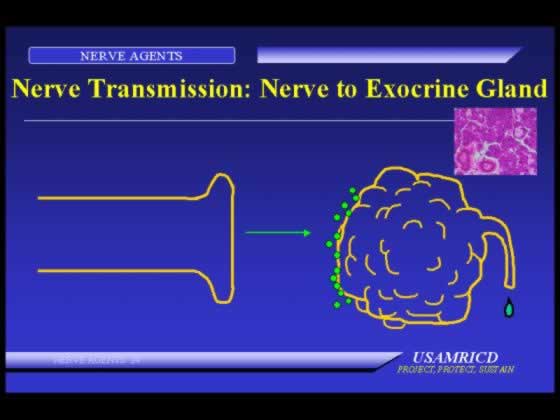
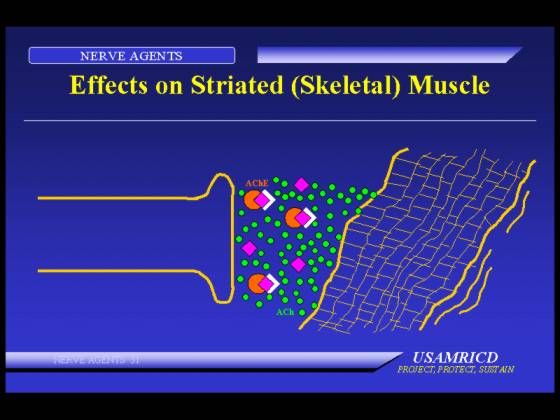
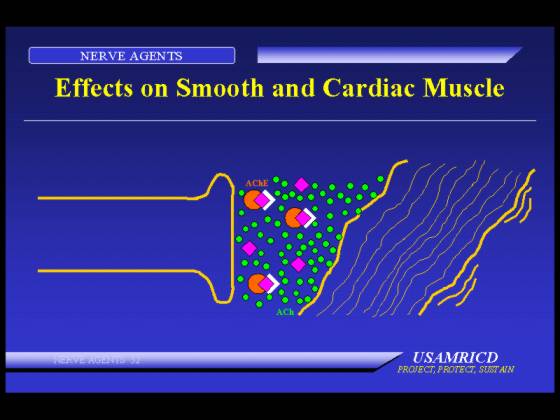
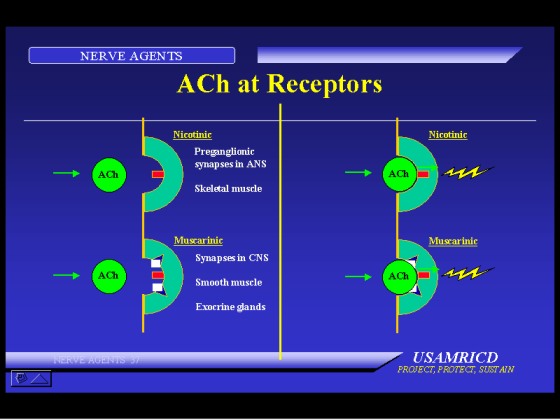
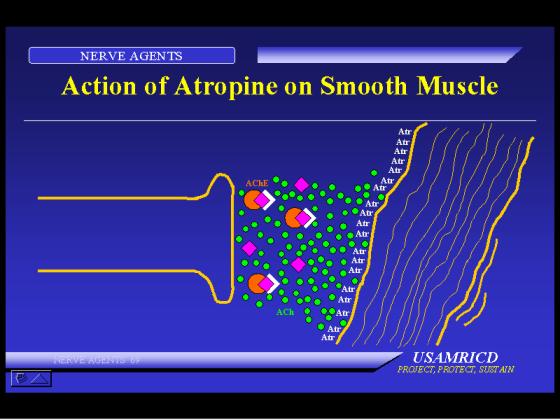
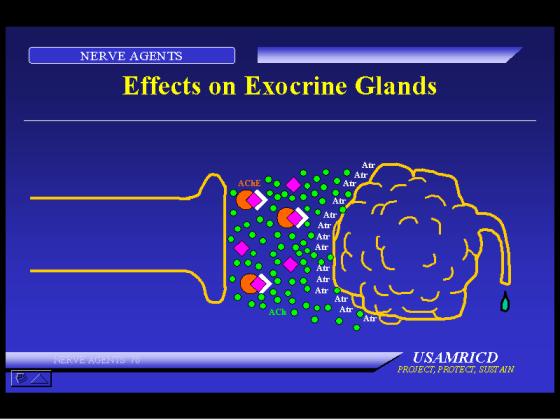
Organs with cholinergic receptor sites include the smooth muscles, skeletal muscles, central nervous system (CNS), and most exocrine glands. In addition, cranial efferents and ganglionic afferents are cholinergic nerves.
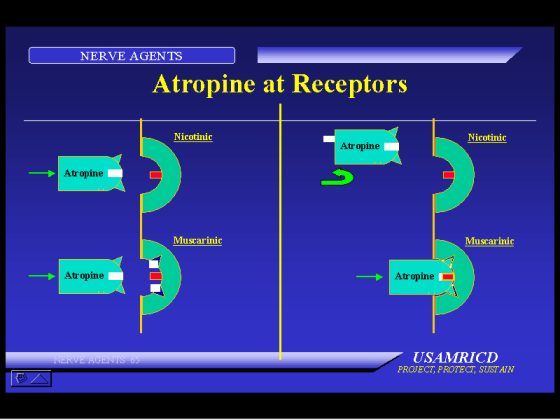
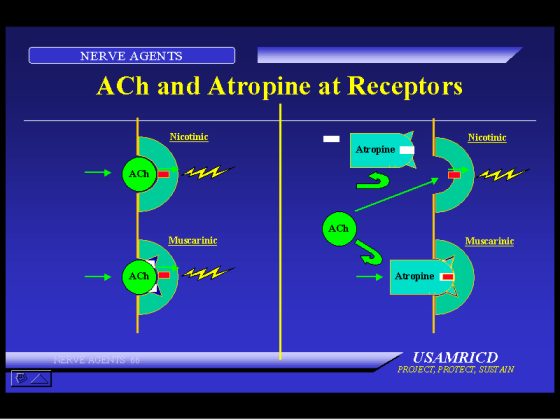
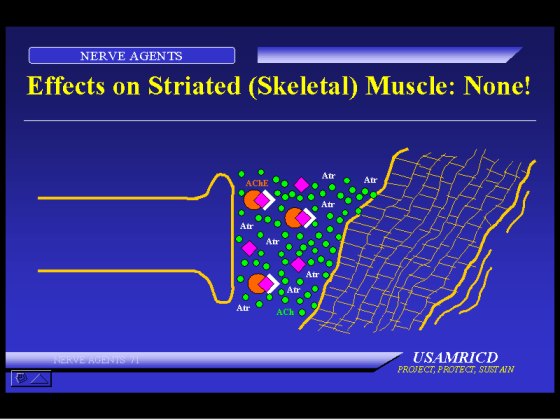
Muscarine will stimulate some of the cholinergic sites, and these are known as muscarinic sites. Organs with these sites include the smooth muscles and glands. Nicotine will stimulate other cholinergic sites, known as nicotinic sites, which are those in skeletal muscle and ganglia. The CNS contains both types of receptors, but the pharmacology in the CNS is more complex and less well understood. Atropine and similar compounds block the effects of excess acetylcholine more effectively at muscarinic sites than at nicotinic sites.
Some commonly used pesticides (for example, the organophosphate (OP) Malathion and the carbamate Sevin) and some common therapeutic drugs (the carbamates pyridostigmine [Mestinon] and physostigmine [Antilirium]) also inhibit acetylcholinesterase and can be considered "nerve agents." However, while the OP pesticides cause the same biological effects as nerve agents, there are some important differences in the duration of biological activity and response to therapy.
The initial effects of exposure to a nerve agent depend on the dose and route of exposure. The initial effects from a sublethal amount of agent by vapor exposure are different than the initial effects from a similar amount of liquid agent on the skin.
Toxicities:The estimated amounts to cause certain effects in man are shown in Tables I and II. In Table I, L indicates lethal, I indicates incapacitating (severe), and M indicates miosis. The large amounts of tabun (GA) and GB required to produce effects after skin application reflect the volatility of these agents. They evaporate rather than penetrate the skin. However, if these agents are occluded and prevented from evaporating, they penetrate the skin very well.
Table I
Vapor Toxicity
mg-min/m3
|
Agent |
LCt50 |
ICt50 |
MCt50 |
|
GA |
400 |
300 |
2-3 |
|
GB |
100 |
75 |
3 |
|
GD |
70 |
UNK |
<1 |
|
GF |
UNK |
UNK |
<1 |
|
VX |
50 |
35 |
0.04 |
Table II
|
Agent |
Amount |
|
GA |
1000 mg |
|
GB |
1700 mg |
|
GD |
50 mg |
|
GF |
30 mg |
|
VX |
10 mg |
Sarin (GB), the agent studied most thoroughly in man, will cause miosis, rhinorrhea, and a feeling of tightness in the throat or chest at a Ct of 3 to 5 mg·min/m3.
Effects: Exposure to a small amount of nerve agent vapor causes effects in the eyes, nose, and airways. These effects are from local contact of the vapor with the organ and do not indicate systemic absorption of the agent. In this circumstance, the erythrocyte-ChE may be normal or depressed. A small amount of liquid agent on the skin causes systemic effects initially in the gastrointestinal (GI) tract. Lethal amounts of vapor or liquid cause a rapid cascade of events culminating within a minute or two with loss of consciousness and convulsive activity, followed by apnea and muscular flaccidity within several more minutes.
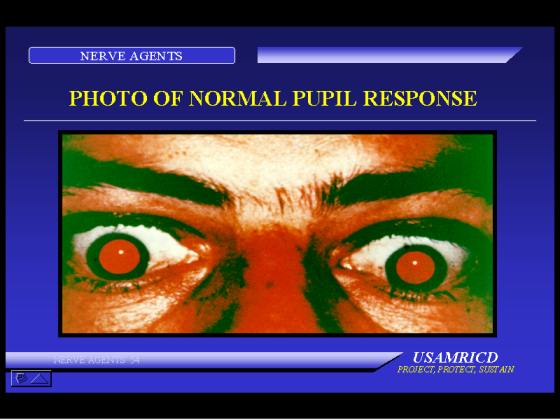
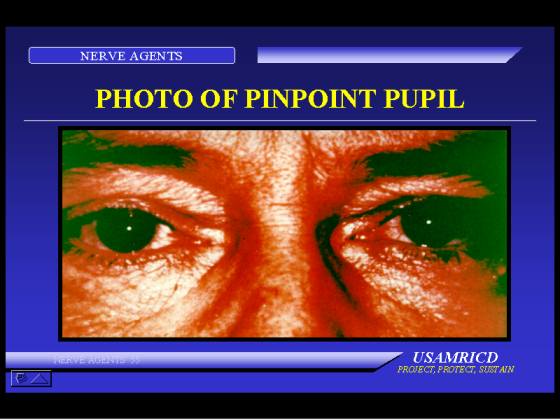
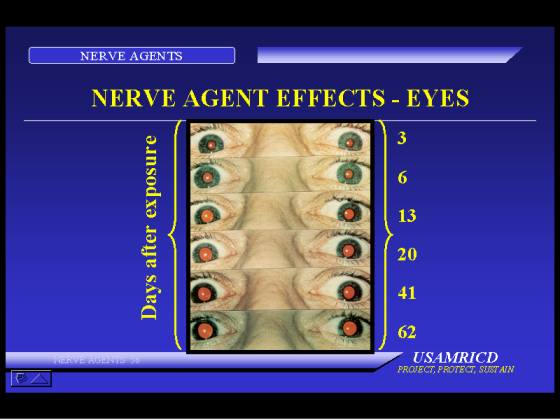
Eye: Miosis is a characteristic sign of exposure to nerve agent vapor. It occurs as a result of direct contact of vapor with the eye. Liquid agent on the skin will not cause miosis if the amount of liquid is small. A moderate amount of liquid may or may not cause miosis. A lethal or near-lethal amount of agent usually causes miosis. A droplet of liquid in or near the eye will also cause miosis. Miosis will begin within seconds or minutes after the onset of exposure to agent vapor, but it may not be complete for many minutes if the vapor concentration is low. Miosis is bilateral in an unprotected individual, but occasionally may be unilateral in a masked person with a leak in his mask eyepiece.
Miosis is often accompanied by complaints of pain, dim vision, blurred vision, conjunctival injection, nausea, and occasionally, vomiting. The pain may be sharp or dull, in or around the eyeball, but more often is a dull ache in the frontal part of the head. Dim vision is due in part to the small pupil, and cholinergic mechanisms in the visual pathways also contribute. The complaint of blurred vision is less easily explained, as objective testing usually indicates an improvement in visual acuity because of the "pin-hole" effect. Conjunctival injection may be mild or severe, and occasionally subconjunctival hemorrhage is present. Nausea (and sometimes vomiting) is part of a generalized complaint of not feeling well. Topical homatropine or atropine in the eye can relieve miosis, pain, dim vision, and nausea.
Nose: Rhinorrhea may be the first indication of nerve agent vapor exposure. Its severity is dose dependent.
Airways: Nerve agent vapor causes bronchoconstriction and increased secretions of the glands in the airways in a dose-related manner. The exposed person may feel a slight tightness in his chest after a small amount of agent and may be in severe distress after a large amount of agent. Cessation of respiration occurs within minutes after the onset of effects from exposure to a large amount of nerve agent. This apnea is probably mediated through the CNS, although peripheral factors (skeletal muscle weakness, e.g., the intercostal muscles, and bronchoconstriction) may contribute
Gastrointestinal (GI) tract: After they are absorbed, nerve agents cause an increase in the motility of the GI tract and an increase in secretions by the glands in the wall of the GI tract. Nausea and vomiting are early signs of liquid exposure on the skin. Diarrhea may occur with large amounts of agent.
Glands: Nerve agent vapor causes increases in secretions from the glands it contacts, such as the lacrimal, nasal, salivary, and bronchial glands. Localized sweating around the site of liquid agent on the skin is common, and generalized sweating after a large liquid or vapor exposure is common. Increased secretions of the glands of the GI tract occur after systemic absorption of the agent by either route.
Skeletal Muscle: The first effect of nerve agents on skeletal muscle is stimulation producing muscular fasciculations and twitching. After a large amount of agent, fatigue and weakness of muscles are rapidly followed by muscular flaccidity.
Fasciculations are sometimes seen early at the site of a droplet of liquid agent on the skin, and generalized fasciculations are common after a large exposure. These may remain long after most of the other acute signs decrease.
Central Nervous System (CNS): The acute CNS signs of exposure to a large amount of nerve agent are loss of consciousness, seizure activity, and apnea. These begin within a minute after exposure to a large amount of agent vapor and may be preceded by an asymptomatic period of 1 to 30 minutes after contact of liquid with the skin.
After exposure to smaller amounts of nerve agents, CNS effects vary and are nonspecific. They may include forgetfulness, an inability to concentrate fully, insomnia, bad dreams, irritability, impaired judgement, and depression. They do not include frank confusion and misperceptions (i.e., hallucinations). These may occur in the absence of physical signs or other symptoms of exposure. After a severe exposure, these symptoms occur upon recovery from the acute severe effects. In either case, they may persist for as long as four to six weeks.
Cardiovascular: The heart rate may be decreased because of stimulation by the vagus nerve, but it is often increased because of other factors such as fright, hypoxia, and the influence of adrenergic stimulation secondary to ganglionic stimulation. Thus, the heart rate may be high, low, or in the normal range. Bradyarrhythmias such as first-, second-, or third-degree heart block may occur. The blood pressure may be elevated from adrenergic factors, but is generally normal until the terminal decline.
Physical findings depend on the amount and route of exposure. After exposure to small to moderate amounts of vapor, there are usually miosis and conjunctival injection, rhinorrhea, and pulmonary signs, although the latter may be absent even in the face of mild to moderate pulmonary complaints. In addition to these signs, an exposure to a high Ct may precipitate copious secretions from the nose and mouth, generalized muscular fasciculations, twitching or seizure activity, loss of consciousness, and apnea. Cyanosis, hypotension, and bradycardia may be present just before death.
Exposure to a small droplet of liquid on the skin may produce few physical findings. Sweating, blanching, and occasionally, fasciculations, at the site may be present soon after exposure, but may no longer be present at the onset of GI effects. After a large exposure, the signs are the same as after vapor exposure.
Miosis is a useful sign of exposure to vapor but does not occur after a liquid exposure unless the amount of exposure is large or the exposure is in or close to the eye.
Effects from nerve agent vapor begin within seconds to several minutes after exposure. Loss of consciousness and onset of seizure activity have occurred within a minute of exposure to a high Ct. After exposure to a very low Ct, miosis and other effects may not begin for several minutes, and miosis may not be complete for 15 to 30 minutes after removal from the vapor. There is no latent period or delay in onset from vapor exposure. Effects may continue to progress for a period of time, but maximal effects usually occur within minutes after exposure stops.
A large amount of liquid on the skin causes effects within minutes. Commonly there is an asymptomatic period of 1 to 30 minutes, and then the sudden onset of an overwhelming cascade of events, including loss of consciousness, seizure activity, apnea, and muscular flaccidity. After small amounts of liquid agent on the skin, the onset of effects has been delayed for as long as 18 hours after contact. These effects are initially gastrointestinal and are usually not life threatening. Generally, the longer the interval, the less severe are the effects.
The effects caused by a mild vapor exposure, namely rhinorrhea and tightness in the chest, may easily be confused with an upper respiratory malady or an allergy. Miosis, if present, will help to distinguish these, but the eyes must be examined in very dim light to detect this. Similarly, GI symptoms from another illness may be confused with those from nerve agent effects, and in this instance there will be no useful physical signs. History of possible exposure will be helpful, and laboratory evidence (decreased RBC-ChE activity), if available, will be useful to distinguish the two.
The diagnosis is easier in the severely intoxicated patient. The combination of miosis, copious secretions, and generalized muscular fasciculations in a gasping, cyanotic, and convulsing patient is characteristic.
Nerve agents inhibit the cholinesterase activity of the blood components, and estimation of this activity is useful in detecting exposure to these agents. The erythrocyte enzyme activity is more sensitive to acute nerve agent exposure than is the plasma enzyme activity.
The amount of inhibition of this enzyme activity does not correlate well with the severity of local effects from mild to moderate vapor exposure. The enzyme activity may be from 0 to 100% of the individual's normal activity in the face of miosis, rhinorrhea, and/or airway symptoms. Normal or nearly normal erythrocyte acetylcholinesterase activity may be present with moderate effects in these organs. At the other extreme, the enzyme may be inhibited by 60 to 70% when miosis or rhinorrhea is the only sign of exposure. Severe systemic effects generally indicate inhibition of the erythrocyte acetylcholinesterase by 70 to 80% or greater.
Other laboratory findings will relate to complications. For example, acidosis may occur after prolonged hypoxia.
Management of a casualty with nerve agent intoxication consists of decontamination, ventilation, administration of the antidotes, and supportive therapy. The condition of the patient dictates the need for each of these and the order in which they are done.
Decontamination is described elsewhere in this manual. Skin decontamination is not necessary after exposure to vapor alone, but clothing should be removed because it may contain "trapped" vapor.
The need for ventilation will be obvious, and the means of ventilation will depend on available equipment. Airway resistance is high (50-70 cm of water) because of bronchoconstriction and secretions, and initial ventilation is difficult. The resistance decreases after atropine administration, after which ventilation will be easier. The copious secretions that may be thickened by atropine also impede ventilatory efforts and require frequent suctioning. In reported cases of severe nerve agent exposure, ventilation has been required from 0.5 to 3 hours.
Three drugs are used to treat nerve agent exposure, and another is used as pretreatment for potential nerve agent exposure. The three therapeutic drugs are atropine, pralidoxime chloride, and diazepam. The use of the pretreatment drug pyridostigmine bromide is discussed later in this chapter.
Atropine is a cholinergic blocking or anticholinergic compound. It is extremely effective in blocking the effects of excess acetylcholine at peripheral muscarinic sites. Under experimental conditions, very large amounts may block some cholinergic effects at nicotinic sites, but these antinicotinic effects are not evident even at high clinical doses. When small amounts (2 mg) are given to normal individuals without nerve agent intoxication, atropine causes mydriasis, a decrease in secretions (including a decrease in sweating), mild sedation, a decrease in GI motility, and tachycardia. The amount in three MARK I Kits may cause adverse effects on military performance in a normal person. In people not exposed to nerve agents, amounts of 10 mg or higher may cause delirium. Potentially, the most hazardous effect of inadvertent use of atropine (2 mg, i.m.) in a young person not exposed to a cholinesterase inhibiting compound in a warm or hot atmosphere is inhibition of sweating, which may lead to heat injury. In the military, atropine is packaged in autoinjectors, each containing 2 mg.
Pralidoxime chloride (Protopam chloride, 2-PAMCl) is an oxime. Oximes attach to the nerve agent that is inhibiting the cholinesterase and break the agent-enzyme bond to restore the normal activity of the enzyme. Clinically, this is noticeable in those organs with nicotinic receptors. Abnormal activity in skeletal muscle decreases and normal strength returns. The effects of an oxime are not apparent in organs with muscarinic receptors; oximes do not cause a decrease in secretions, for example. They also are less useful after aging occurs, but with the exception of GD (soman) intoxicated individuals, casualties will be treated before significant aging occurs.
Pralidoxime chloride (600 mg) is in an autoinjector for self-use along with the atropine injector. These atropine and pralidoxime chloride autoinjectors are packaged together in a MARK I Kit. Each soldier is issued three MARK I Kits.
Diazepam is an anticonvulsant drug used to decrease convulsive activity and reduce the brain damage caused by prolonged seizure activity. Without the use of pyridostigmine pretreatment, experimental animals died quickly after superlethal doses of nerve agents despite conventional therapy. With pyridostigmine pretreatment (followed by conventional therapy), animals survived superlethal doses of soman but had prolonged periods of seizure activity before recovery. They later had performance decrements and anatomic lesions in their brains. The administration of diazepam with other standard therapy to soman-poisoned animals pretreated with pyridostigmine reduced the seizure activity and its sequelae. Current military doctrine is to administer diazepam with other therapy (three MARK I Kits) at the onset of severe effects from a nerve agent, whether or not seizure activity is among those effects. Each soldier carries one autoinjector containing 10 mg of diazepam for his buddy to administer to him (if he could self-administer it, he would not need it). Diazepam should be administered with the three MARK I Kits when the casualty's condition warrants the use of three kits at the same time. Medical personnel can administer more diazepam to a casualty if necessary. The medical corpsman carries extra diazepam injectors and is authorized to administer two additional injectors at ten-minute intervals to a convulsing casualty.
The doctrine for self-aid for nerve agent intoxication states that if an individual has effects from the agent, he/she should self-administer one MARK I Kit. If there is no improvement in ten minutes, he/she should seek out a buddy to assist in the evaluation of his/her condition before further MARK I Kits are given. If a buddy finds an individual severely intoxicated (e.g., gasping respirations, twitching, etc.) so that the individual cannot self-administer a MARK I Kit, the buddy should administer three MARK I Kits and diazepam immediately. The discussion below is advice for medical assistance.
The appropriate number of MARK I Kits to administer initially to a casualty from nerve agent vapor depends on the severity of the effects. Systemic atropine will not reverse miosis (unless administered in very large amounts), and miosis alone is not an indication for a MARK I Kit. If the eye or head pain and nausea associated with the miosis are severe, topical application of atropine (or homatropine) in the eye will bring relief. Topical atropine should not be used without good reason (severe pain), because it causes blurred vision for a day or longer. A casualty with miosis and rhinorrhea should be given one MARK I Kit only if the rhinorrhea is severe and troublesome (he cannot keep his mask on because of fluid). A casualty with mild to moderate dyspnea should be given one or two MARK I Kits, depending on the severity of his distress and the time between exposure and therapy. Some of the respiratory distress from a mild exposure will spontaneously decrease within 15 to 30 minutes after termination of exposure, so if the casualty is not severely uncomfortable, only one MARK I Kit should be used initially. Atropine is quite effective, and care should be taken not to give too much in a casualty who does not need it.
A severe casualty from nerve agent vapor has miosis, copious secretions from the nose and mouth, severe difficulty breathing or apnea, possibly some degree of cyanosis, muscular fasciculations, and twitching or convulsive activity, and is unconscious. He should be given three MARK I Kits and diazepam immediately. Ventilation will be needed and should be done via an endotracheal airway if possible. Suctioning of the excessive airway secretions will be necessary to enhance air exchange and will make ventilatory efforts easier. Atropine, 2 mg, should be repeated at three to five-minute intervals and should be titrated to a reduction of secretions and to reduction of ventilatory resistance. When the intravenous preparation is available, the preferred route of atropine administration is via the intravenous route, but this route should be avoided until hypoxia is corrected, because intravenously administered atropine in hypoxic animals has produced ventricular fibrillation. In a hypotensive patient or a patient with poor veins, atropine might be given intratracheally, either via the endotracheal tube or directly into the trachea, for more rapid absorption via the peribronchial vessels.
The medical care provider might err in giving too much atropine to a mild to moderate casualty. More importantly, the care provider might err by giving too little atropine to a severe casualty. In a severe casualty, atropine should be pushed at frequent intervals until secretions are dry (or nearly dry) and until ventilation can be accomplished with ease. In reported cases this has required 10 to 20 mg of atropine within the first several hours. A conscious, less-severely exposed casualty should receive atropine until he is breathing comfortably, and he will be able to communicate this. Dry secretions need not be an endpoint in mild to moderate casualties.
The casualty with skin exposure to liquid is more difficult to evaluate and manage than is a vapor exposure casualty. Agent on the surface of the skin can be decontaminated, but agent absorbed into the skin cannot be removed. The initial effects from absorbed liquid agent can start two to three hours after thorough decontamination of agent droplets on the skin. A casualty from liquid exposure on the skin may continue to worsen because of continued absorption of the agent from the skin depot.
The first effects of a liquid droplet on the skin are sweating with or without blanching, and occasionally, muscular fasciculations at the site. Gastrointestinal effects (nausea, vomiting, and sometimes diarrhea) are the first systemic effects, and these may start from 0.5 to 18 hours after contact with the agent. If these effects occur within the first several hours after exposure, they may portend more severe effects, and initial therapy should be two MARK I Kits. If effects begin later, initial therapy should be one MARK I Kit.
A large amount of liquid agent on the skin will cause effects 1 to 30 minutes after contact, whether or not decontamination was done. Nevertheless, early decontamination may lessen the magnitude of the effects. After a 1 to 30-minute latent or asymptomatic period, the casualty will suddenly lose consciousness and begin seizure activity. The condition of the casualty and management are the same as described for a severe casualty from vapor exposure.
Further care of the severe casualty consists of atropine administration to minimize secretions and ventilation until spontaneous respiration resumes. Oxime administration should be repeated at hourly intervals for two or three additional doses. The preferred method of administration of the oxime is by intravenous drip of 1 gram over 20 to 30 minutes (more rapid administration will cause hypertension), but 3 additional oxime autoinjectors (total dose of 1.8 grams) may be given if the intravenous route cannot be used. The need for ventilation may continue for 0.5 to 3 hours. Unless prolonged hypoxia or other complications have occurred, the casualty will eventually begin having spontaneous muscular activity and make sporadic attempts to breathe. Muscles will become stronger and breathing more regular, and the casualty will have intermittent episodes of conscious behavior. Within an hour or two, he will be breathing, moving, and conscious, although he will be weak and intermittently obtunded.
Vapor Exposure
Mild
· Eyes: miosis, dim vision, headache
· Nose: rhinorrhea
· Mouth: salivation
· Lungs: dyspnea ("tightness in the chest")
· Time of onset: seconds to minutes after exposure
· Self-aid: one MARK I Kit
· Buddy-aid: stand by
Severe
· All of the above, plus
· Severe breathing difficulty or cessation of respiration
· Generalized muscular twitching, weakness, or paralysis
· Convulsions
· Loss of consciousness
· Loss of bladder, bowel control
· Time of onset: seconds to minutes after exposure
· Self-aid: None - soldier will be unable to help self
· Buddy-aid: 3 MARK I Kits and diazepam immediately
Liquid on Skin
Mild/moderate
· Muscle twitching at site of exposure
· Sweating at site of exposure
· Nausea, vomiting
· Feeling of weakness
· Time of onset: 10 minutes to 18 hours after exposure
· Self-aid: one to two MARK I Kits, depending on severity of symptoms
· Buddy-aid: stand by
Severe
All of the above, plus
· Severe breathing difficulty or cessation of breathing
· Generalized muscular twitching, weakness, or paralysis
· Convulsions
· Loss of consciousness
· Loss of bladder and bowel control
· Time of onset: minutes to an hour after exposure
· Self-aid: none - soldier will be unable to help himself
· Buddy-aid: three MARK I Kits and diazepam immediately
In late 1990, the United States military fielded pyridostigmine bromide as a pretreatment for nerve agent exposure. Each individual received a blister pack containing twenty-one 30-mg tablets. The dose regimen is one 30-mg tablet every eight hours. When to start and stop dosing is a division or corps' command decision and is made with the advice of the intelligence, chemical, and medical staffs. To use or to stop the pretreatment is not a local decision, nor is it an individual decision.
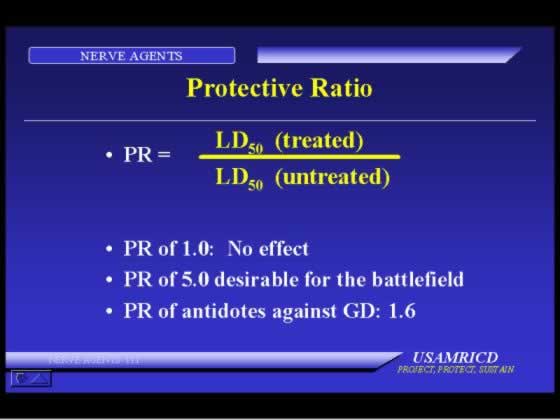
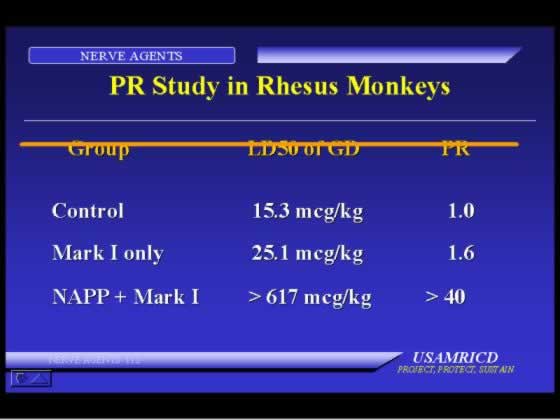
When given before soman exposure and when that exposure is followed by the standard MARK I therapy, the use of pretreatment will increase the LD50 several fold over the LD50 obtained without the use of the pretreatment. When soman is the nerve agent, the use of pyridostigmine increases survival. When the agent is GB or VX, survival after standard MARK I therapy is essentially the same whether or not pyridostigmine pretreatment is used, i.e., pyridostigmine use provides no benefit in GB or VX poisoning. Current data are not adequate to evaluate the effectiveness of pyridostigmine pretreatment for GA or GF exposure.
Pyridostigmine is not an antidote, and it should not be taken after soman exposure. Its use will not decrease the effects of soman. It is ineffective unless standard MARK I therapy is also used in the appropriate manner.
One consequence of the greater survival from the use of pyridostigmine is prolonged seizure activity and subsequent brain damage in the survivors. The early administration of diazepam will decrease these effects.
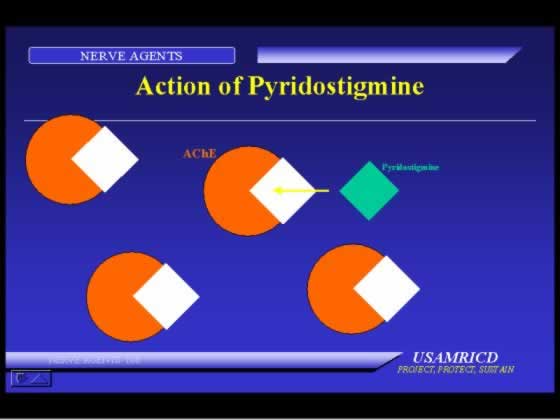
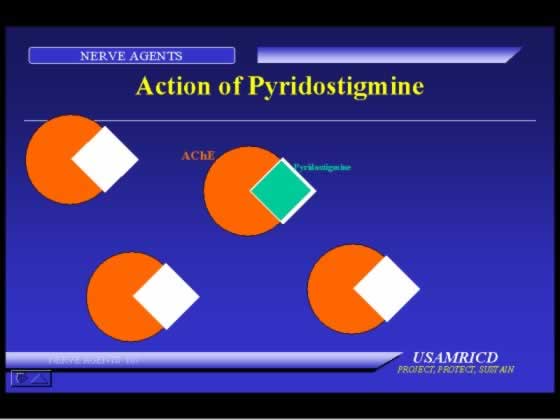
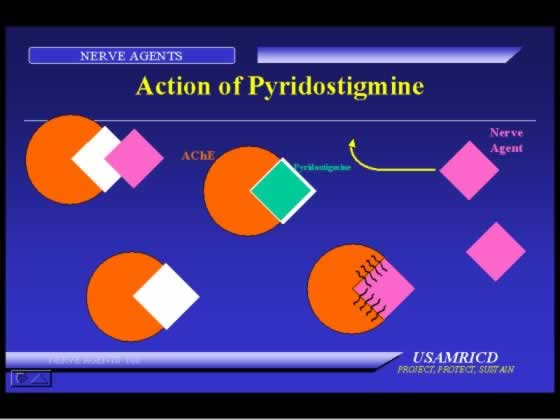
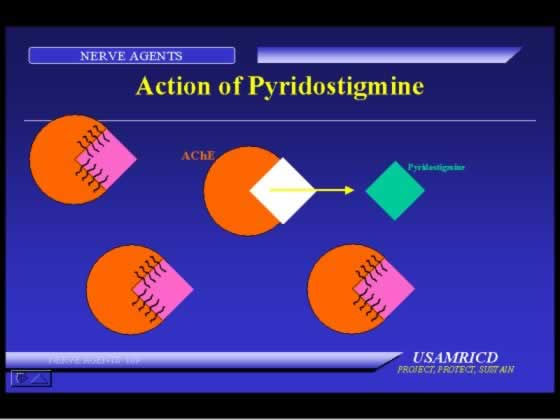
About 50 years ago, it was noted that carbamates bind to the active site of cholinesterase in a similar manner to the binding of organophosphorus cholinesterase inhibitors to cholinesterase. Additionally, while the carbamate was attached to the active site, an organophosphorus compound could not attach to the enzyme. The carbamate-enzyme binding, or carbamylation, lasts only for hours, rather than for the lifetime of the enzyme as the organophosphorus compound attachment does. While the enzyme is carbamylated, the active site is protected from attack by other compounds such as organophosphorous cholinesterase inhibitors, including nerve agents. After several hours, the carbamate leaves the enzyme (that is, decarbamylation occurs), and the enzyme becomes completely functional again. Thus, the carbamate provides temporary protection for the enzyme against nerve agent attack.
Over the past several decades, many carbamates have been investigated for their effectiveness in animals and their safety in man. Pyridostigmine was chosen and underwent extensive testing in humans. Investigations indicated that it did not interfere with the performance of military tasks and caused no adverse physiological disturbances. The incidence of side effects from the drug during these studies was reported as fewer than 5%.
ISRAELI STUDY
Tens of thousands of United States troops took pyridostigmine during the recent Gulf War Conflict. The incidence of side effects (primarily gastrointestinal and urinary) was over 50%, but only a few percent of the troops sought medical help because of the severity of these effects. The drug was discontinued in less than 1% of cases.
A severe nerve agent casualty who is unconscious, convulsing or post-ictal, breathing with difficulty or apneic, and possibly flaccid will survive with appropriate, immediate therapy (including ventilation) if he still has an intact circulation. He should be triaged as immediate if that therapy can be provided. If a blood pressure cannot be obtained, he should be considered expectant.
The casualty with severe symptoms who is spontaneously breathing, has not lost consciousness, and has not seized has an excellent chance of survival with a minimal amount of therapeutic effort. He should be categorized as immediate and given three MARK I Kits and diazepam. He may worsen if his exposure was to liquid, and atropine administration should be repeated at frequent intervals. If he loses consciousness, seizes, and becomes apneic, he will be retriaged, and his further care will depend on available resources.
Casualties who are walking and talking will usually be triaged as minimal. If a casualty can walk and talk, he is breathing and his circulation is intact. He would not appear to need immediate, life-saving care. This does not preclude self-administration or medic-administration of further antidotes for symptoms, and these should be given as necessary.
A casualty recovering from a severe exposure who has received large amounts of antidotes and has been ventilated will be triaged as delayed, because he is in need of further medical observation or care.
Return to duty depends on the status of the casualty, his military assignment, and the tactical situation.
Studies indicate that animals with decreased erythrocyte acetylcholinesterase activity from a nerve agent exposure have a decreased LD50 for another nerve agent exposure (they are more susceptible to the agent) until that cholinesterase activity returns to at least 75% of its baseline, or pre-exposure activity. Nerve agent exposed workers in a depot or research facility are prevented from returning to work with agents until this recovery occurs. In a battlefield situation, this conservative management should be balanced against the need for the person and his risk of being exposed to a large amount of agent.
In a military field situation, the capability to analyze blood for erythrocyte cholinesterase activity is usually not available, and the "normal" or baseline activity of each individual is not known. The erythrocyte cholinesterase activity in a casualty with severe systemic effects will be inhibited by 70% or greater (30% or less of his pre-exposure activity), and 45 days or longer will be required for cholinesterase activity to return to 75% of pre-exposure activity. The enzyme activity of a casualty with mild or moderate effects from agent vapor might be nearly normal or might be markedly inhibited. A prediction of erythrocyte cholinesterase recovery time is unreliable.
Most individuals triaged as minimal could return to duty within several hours if the tactical situation required all available manpower. The lingering ocular and CNS effects may be limiting factors in these cases. These individuals might be able to fire a rifle, but their performance on a tracking screen might be severely decremented because of both visual problems and difficulty in concentrating. These prolonged effects must be thoroughly evaluated before the casualties are returned to duty. Whether these individuals should be evacuated to a facility with the capability for analysis of erythrocyte cholinesterase activity and retained there until the activity returns will be dictated by the tactical situation.
A casualty who has had severe effects might be walking and talking after 6 to 24 hours but will still be unfit for most duties. Ideally, he should be kept under medical observation for a week or longer and not returned until recovery of cholinesterase activity. However, the tactical situation may lead to modification of these guidelines.
Minor electroencephalographic changes were noted more than a year after nerve agent exposure when averaged EEGs in a group of people who had been exposed to a nerve agent were compared to a control group. Changes could not be identified in individuals. Neuropsychiatric changes have been noted in individuals for weeks to months after exposure to insecticides.
Polyneuropathy, reported after OP insecticide poisoning, has not been reported in humans exposed to nerve agents and has been produced in animals only at doses of nerve agents so high that survival would be unlikely. The Intermediate Syndrome has not been reported in humans after nerve agent exposure, nor has it been produced in animals by nerve agent administration. Muscular necrosis has been produced in animals after high dose nerve agent exposure but reverses within weeks; it has not been reported in humans.
|
Introduction |
Nerve Agents |
||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}